■ 試験デザイン
TPECOに分けると下記のようになります
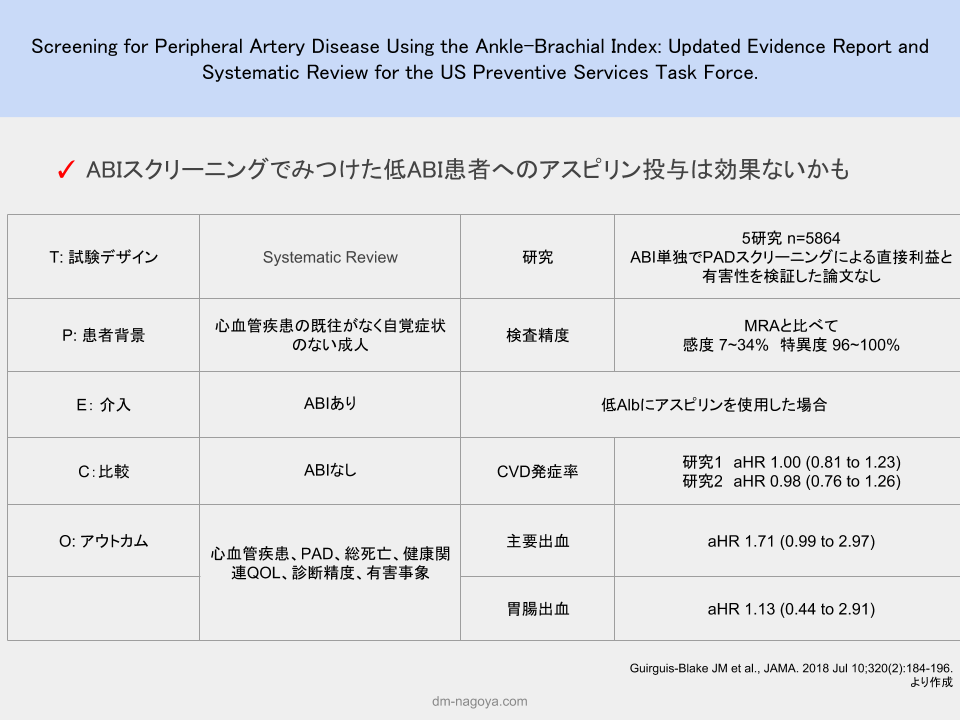
T: 試験デザイン Systematic Review
P: 患者背景 心血管疾患の既往がなく自覚症状のない成人
E: 介入 ABIあり
C:比較 ABIなし
O: アウトカム 心血管疾患、PAD、総死亡、健康関連QOL、診断精度、有害事象
■ 結果
No population-based screening trials evaluated the direct benefits or harms of PAD screening with the ABI alone. A single diagnostic accuracy study of the ABI compared with magnetic resonance angiography gold-standard imaging (n = 306) found low sensitivity (7%-34%) and high specificity (96%-100%) in a screening population. Two adequately powered trials (n = 4626) in asymptomatic populations with and without diabetes with a variably defined low ABI (≤0.95 or ≤0.99) showed no statistically significant effect of aspirin (100 mg daily) for composite CVD outcomes (adjusted hazard ratio [HR], 1.00 [95% CI, 0.81-1.23] and HR, 0.98 [95% CI, 0.76-1.26]). One trial (n = 3350) demonstrated no statistically significant increase in major bleeding events with the use of aspirin (adjusted HR, 1.71 [95% CI, 0.99- 2.97]) and no statistically significant increase in major gastrointestinal bleeding (relative risk, 1.13 [95% CI, 0.44-2.91]).
ABIは脚の血圧と腕の血圧を比較して、動脈硬化をみる検査です。
通常であれば、脚の血圧>腕の血圧ですが、動脈硬化がすすむと長い血管ほど狭くなっているので
脚の血圧<腕の血圧となります。
これを利用して、糖尿病患者さんではABI/TBIによるスクリーニングを行うことがあるのですが、効果については疑問なところでした。
今回の結果からUSPSTFはABIは有効性および有害性を判断するにはエビデンス不足(文献2)と報告しています。
個人的には、症状がない場合には低ABIでもアスピリンのCVD予防効果がないことがわかったのが大きいです。
また、糖尿病患者さんではABIはうまく動脈硬化を反映しないので、TBIのほうが望ましいとされているため。TBIの予防効果がわかれば、より治療の参考になりますね。
■ 参照文献
Guirguis-Blake JM et al., JAMA. 2018 Jul 10;320(2):184-196.
PMID: 29998343
文献2
US Preventive Services Task Force., JAMA. 2018 Jul 10;320(2):177-183.
PMID: 29998344