■ 試験デザイン
TPECOに分けると下記のようになります
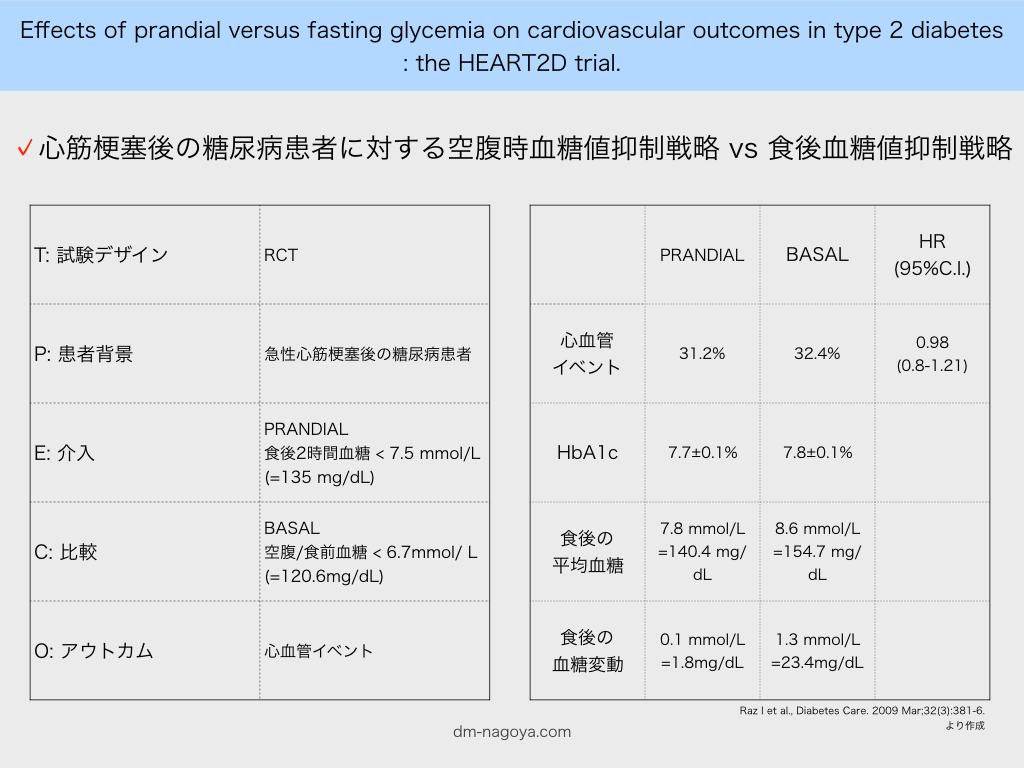
T RCT
P 急性心筋梗塞後の糖尿病患者
E 食後2時間血糖 < 7.5 mmol/L(=135 mg/dL)
C 空腹/食前血糖 < 6.7mmol/ L(=120.6mg/dL)
O 心血管イベント
■ 結果
The trial was stopped for lack of efficacy. Risks of first combined adjudicated primary cardiovascular events in the PRANDIAL (n = 174, 31.2%) and BASAL (n = 181, 32.4%) groups were similar (hazard ratio 0.98 [95% CI 0.8-1.21]). Mean A1C did not differ between the PRANDIAL and BASAL groups (7.7 +/- 0.1 vs. 7.8 +/- 0.1%; P = 0.4) during the study. The PRANDIAL group showed a lower daily mean postprandial blood glucose (7.8 vs. 8.6 mmol/l; P < 0.01) and 2-h postprandial blood glucose excursion (0.1 vs. 1.3 mmol/l; P < 0.001) versus the BASAL group.
■ 副作用
The incidence of hypoglycemia (all) was similar between groups through visit 8 (when this information was collected) (PRANDIAL versus BASAL: 55.3 vs. 55.2%; P = 0.367), and the incidence of severe hypoglycemia was also similar throughout the trial (PRANDIAL versus BASAL: 12.9 vs. 9.5%; P = 0.071). The incidence of nocturnal hypoglycemia (through visit 8), however, was greater in the BASAL group than in the PRANDIAL group (10.6 vs. 6.1%; P = 0.007).
低血糖全体および重症低血糖の頻度はPRANDIALとBASALで変わらないものの、夜間低血糖はBASALのほうが多かったというのは、
夜間以外での低血糖がPRANDIALでは多かったということでしょうか。
この試験ではBASALでも食後血糖値154.7mg/dL、血糖変動23.4mg/dLと変動幅がかなり狭くなっております。
臨床では、BASAL治療で空腹時はよいものの、食後血糖値は200や250mg/dLを超える場合に悩むことが多いので、本研究だけで判断するのは難しいところです。少なくとも食後の血糖値が150mg/dl程度で落ち着いている方に関しては、利便性もかんがえてBASAL戦略がよいように思います。
■ 参照文献
Raz I et al., Diabetes Care. 2009 Mar;32(3):381-6. PMID: 19246588