■ 試験デザイン
In July 2014, we searched the MEDLINE and Cochrane databases for English-language articles pertaining to metformin, kidney disease, and lactic acidosis in humans between 1950 and June 2014. We excluded reviews, letters, editorials, case reports, small case series, and manuscripts that did not directly pertain to the topic area or that met other exclusion criteria. Of an original 818 articles, 65 were included in this review, including pharmacokinetic/metabolic studies, large case series, retrospective studies, meta-analyses, and a clinical trial.
TPECOに分けると下記のようになります
T システマティックレビュー
P 非糖尿病 糖尿病
E&C 腎機能
O メトホルミンクリアランス、血中濃度、乳酸アシドーシス発症頻度
■ 結果
Although metformin is renally cleared, drug levels generally remain within the therapeutic range and lactate concentrations are not substantially increased when used in patients with mild to moderate chronic kidney disease (estimated glomerular filtration rates, 30-60 mL/min per 1.73 m2). The overall incidence of lactic acidosis in metformin users varies across studies from approximately 3 per 100,000 person-years to 10 per 100,000 person-years and is generally indistinguishable from the background rate in the overall population with diabetes. Data suggesting an increased risk of lactic acidosis in metformin-treated patients with chronic kidney disease are limited, and no randomized controlled trials have been conducted to test the safety of metformin in patients with significantly impaired kidney function. Population-based studies demonstrate that metformin may be prescribed counter to prevailing guidelines suggesting a renal risk in up to 1 in 4 patients with type 2 diabetes mellitus–use which, in most reports, has not been associated with increased rates of lactic acidosis. Observational studies suggest a potential benefit from metformin on macrovascular outcomes, even in patients with prevalent renal contraindications for its use.
- メトホルミンクリアランスは腎機能低下に伴い低下する
- しかしeGFR30以上であれば、メトホルミン血中濃度は治療域にとどまり、血中乳酸値に有意な影響を与えない
- メトホルミンによる乳酸アシドーシスの頻度は約3~10 / 100,000人年程度であり、糖尿病患者全体の発症率と変わらない
- 慢性腎臓病のメトホルミン治療患者における乳酸アシドーシスのリスク増加を示唆するデータは限られている
- ランダム化比較試験は行われていない。
- 観察研究は、大規模な腎臓禁忌患者であっても、大血管の結果に対するメトホルミンの潜在的な利益を示唆している。
- 人口ベースの研究において、腎機能リスクがある糖尿病患者の4人に1人はメトホルミンが使用されているが、多くは乳酸アシドーシスを増やさないと報告されている。
- 観察研究では腎機能禁忌例でも、心血管イベントに対して有効である可能性が示唆されている
##メトホルミン禁忌 各国比較##
日本(Recommendation2014)
中等度以上の腎機能障害者(だいたいCcr=30∼50mL/min)では禁忌
男性sCr >=1.3mg/dl, 女性sCr >=1.2mg/dlでは推奨しない
75歳以上ではより慎重
FDA
male Cr >=1.5 mg/dl, female Cr >=1.4 mg/dl
abnormal CrCl
80歳以上でCrCl測定せずに開始すること
UK
Cr >=1.7 mg/dL
eGFR <=30
The European Medicines Agency stipulates
eGFR< 60 The Canadian Diabetes Association eGFR> 60 a maximum dose=1700 mg/day
eGFR30~60 a maximum dose=850 mg/day
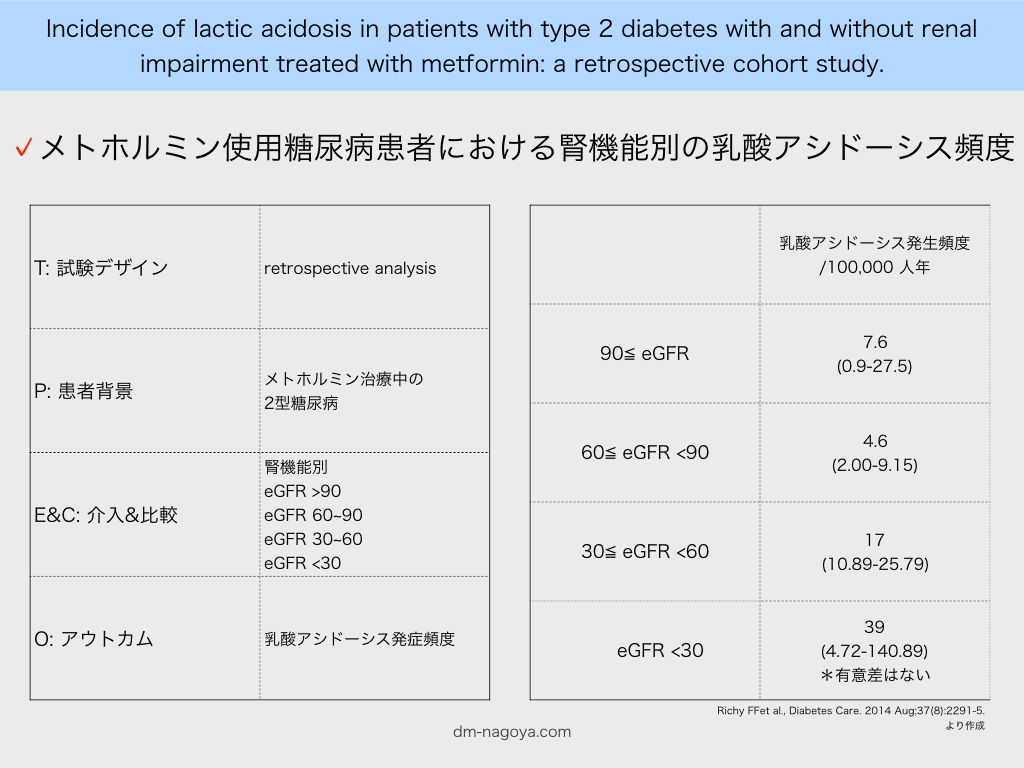
また文献2によると、メトホルミン使用糖尿病患者における腎機能別の乳酸アシドーシス頻度は以下のように報告されています。
eGFR >90 7.6 / 100,000
eGFR 60~90 4.6 / 100,000
eGFR 30~60 17 / 100,000
eGFR *メトホルミン非内服例との比較はなし*
■ 参照文献
Inzucchi SE et al., JAMA. 2014 Dec 24-31;312(24):2668-75. PMID: 25536258
文献2
Richy FF et al., Diabetes Care. 2014 Aug;37(8):2291-5. PMID: 24879835