■ 試験デザイン
TPECOに分けると下記のようになります
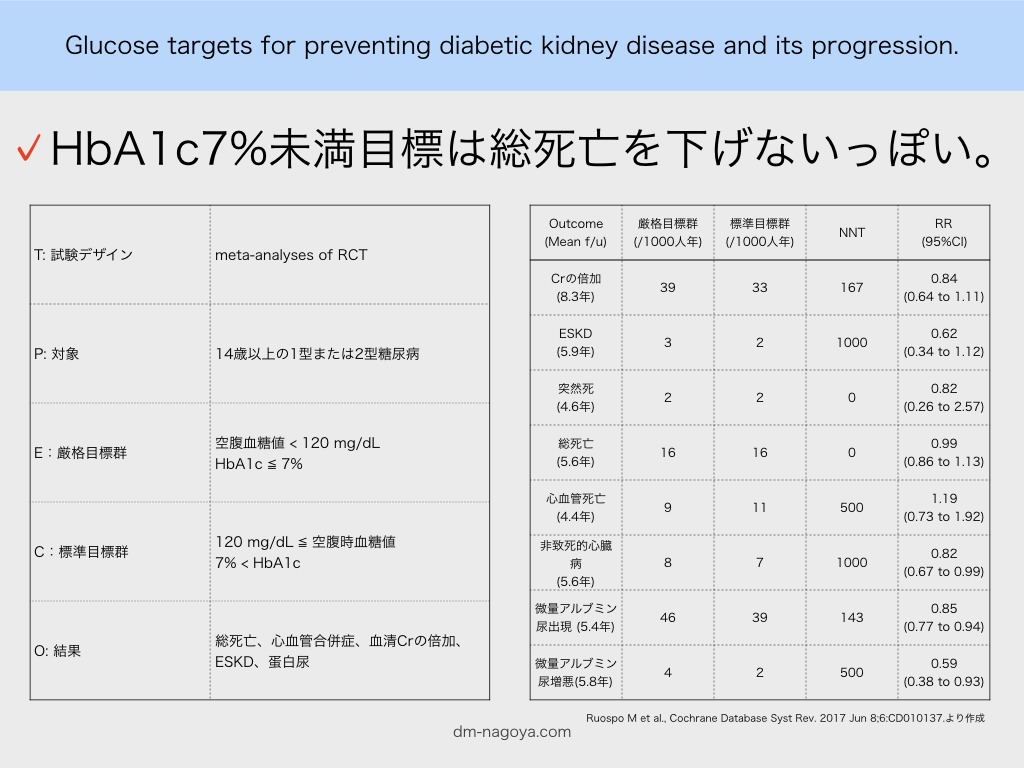
T: meta-analyses of RCT
P: 14歳以上の1型または2型糖尿病
E:厳格目標群 空腹血糖値 < 120 mg/dL HbA1c ≦ 7%
C:標準目標群 120 mg/dL ≦ 空腹時血糖値 7% < HbA1c
O: 結果 総死亡、心血管合併症、血清Crの倍加、ESKD、蛋白尿
■ 結果
MAIN RESULTS:
Fourteen studies involving 29,319 people with diabetes were included and 11 studies involving 29,141 people were included in our meta-analyses. Treatment duration was 56.7 months on average (range 6 months to 10 years). Studies included people with a range of kidney function. Incomplete reporting of key methodological details resulted in uncertain risks of bias in many studies. Using GRADE assessment, we had moderate confidence in the effects of glucose lowering strategies on ESKD, all-cause mortality, myocardial infarction, and progressive protein leakage by kidney disease and low or very low confidence in effects of treatment on death related to cardiovascular complications and doubling of serum creatinine (SCr).For the primary outcomes, tight glycaemic control may make little or no difference to doubling of SCr compared with standard control (4 studies, 26,874 participants: RR 0.84, 95% CI 0.64 to 1.11; I2= 73%, low certainty evidence), development of ESKD (4 studies, 23,332 participants: RR 0.62, 95% CI 0.34 to 1.12; I2= 52%; low certainty evidence), all-cause mortality (9 studies, 29,094 participants: RR 0.99, 95% CI 0.86 to 1.13; I2= 50%; moderate certainty evidence), cardiovascular mortality (6 studies, 23,673 participants: RR 1.19, 95% CI 0.73 to 1.92; I2= 85%; low certainty evidence), or sudden death (4 studies, 5913 participants: RR 0.82, 95% CI 0.26 to 2.57; I2= 85%; very low certainty evidence). People who received treatment to achieve tighter glycaemic control probably experienced lower risks of non-fatal myocardial infarction (5 studies, 25,596 participants: RR 0.82, 95% CI 0.67 to 0.99; I2= 46%, moderate certainty evidence), onset of microalbuminuria (4 studies, 19,846 participants: RR 0.82, 95% CI 0.71 to 0.93; I2= 61%, moderate certainty evidence), and progression of microalbuminuria (5 studies, 13,266 participants: RR 0.59, 95% CI 0.38 to 0.93; I2= 75%, moderate certainty evidence).
今までの試験結果と矛盾しない印象です。
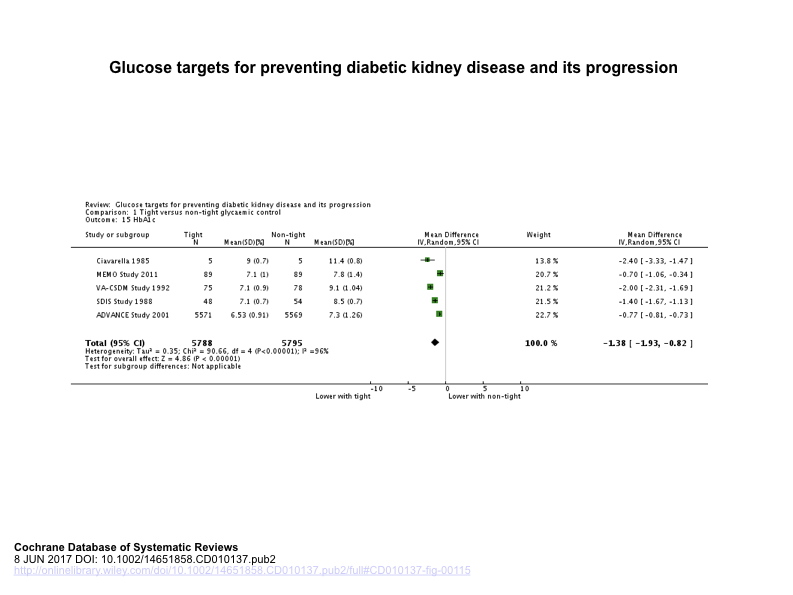
標準治療群の設定がHbA1c > 7%となっており、標準治療群の平均HbA1cがどれくらいだったのか知りたくて、39ドルだして本文を購入しました。
しかし残念ながら、本文中にもメタアナリシス全体の達成HbA1c比較はのっておらず、メタアナリシス全体での厳格目標群HbA1cと標準目標群HbA1cの差が-1.38%(-1.93 to -0.82)であることと、各試験の平均HbA1cが載っているだけでした。
糖尿病発症からESKDになるまで20年ほどかかるという時間軸のなかで、
・このメタアナリシスはOutcomeの平均f/u期間がいずれも10年未満であることをどのように評価すべきか?
・HbA1c < 7%を目指さないとして、目標のHbA1cをどのあたりに設定するか。
このあたりの評価しつつ、目標HbA1cや糖尿病以外のリスクコントロール因子を調節していくところが私の仕事です。
■ 参照文献
Ruospo M et al., Cochrane Database Syst Rev. 2017 Jun 8;6:CD010137.
PMID: 28594069